

Description
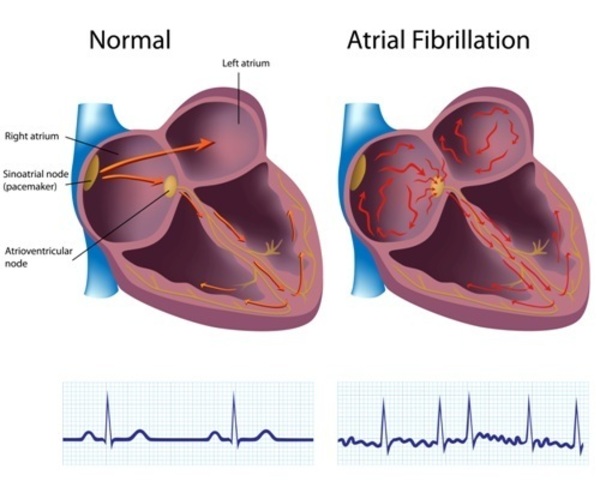
An aldosterone-producing adenoma is a noncancerous (benign) tumor that develops in an adrenal gland, which is a small hormone-producing gland located on top of each kidney. In most cases, individuals develop a single tumor in one of the adrenal glands. The adrenal tumor produces too much of the hormone aldosterone, which is a condition known as primary hyperaldosteronism. Aldosterone helps regulate the body's fluid levels and blood pressure by controlling the amount of salt retained by the kidneys. Excess aldosterone causes the kidneys to retain more salt than normal, which increases the body's fluid levels and blood pressure. People with an aldosterone-producing adenoma may develop severe high blood pressure (hypertension), and they have an increased risk of heart attack, stroke, or an irregular heart beat (atrial fibrillation).
Frequency
Aldosterone-producing adenomas cause up to 60 percent of cases of primary hyperaldosteronism. It is estimated that primary hyperaldosteronism accounts for 5 to 15 percent of cases of hypertension, which affects approximately 3 in 10 adults worldwide. However, the prevalence of aldosterone-producing adenomas is unknown.
Causes
Aldosterone-producing adenomas are caused by mutations in one of several genes. The most commonly mutated gene is KCNJ5, accounting for an estimated 40 percent of the tumors, followed by the CACNA1D and ATP1A1 genes, which are mutated in about 9 percent and 6 percent of aldosterone-producing adenomas, respectively. Changes in other genes cause a small percentage of cases. Only about 60 percent of affected individuals have a mutation in one of the identified genes; additional unidentified genes are also thought to be involved in the condition.
The genes known to be involved in aldosterone-producing adenomas have roles in balancing the amounts of positively charged atoms (ions) of sodium (Na+), potassium (K+), and calcium (Ca2+) in cells. Each of the proteins produced from these genes transports certain ions across cell membranes. The flow of these ions creates an electrical charge across the cell membrane, which affects certain biochemical processes. In adrenal gland cells, this flow of ions helps control the production of aldosterone. Mutations in the KCNJ5, CACNA1D, or ATP1A1 gene lead to abnormal electrical charges across cell membranes. These abnormalities overactivate a biochemical process that increases adrenal cell growth and division (proliferation), which promotes adenoma formation. Overactivation of this biochemical process also increases aldosterone production, resulting in hyperaldosteronism and leading to hypertension.
Inheritance
Aldosterone-producing adenomas are generally not inherited but arise from a mutation in the body's cells that occurs after conception. In particular, the alteration occurs in adrenal gland cells that give rise to the tumor. Such mutations are called somatic mutations.
Other Names for This Condition
- Aldosterone-secreting adenoma
- Aldosteronoma
- Conn adenoma
- Primary aldosteronism due to Conn adenoma
Additional Information & Resources
Genetic Testing Information
Patient Support and Advocacy Resources
Clinical Trials
Scientific Articles on PubMed
References
- Akerstrom T, Maharjan R, Sven Willenberg H, Cupisti K, Ip J, Moser A, Stalberg P, Robinson B, Alexander Iwen K, Dralle H, Walz MK, Lehnert H, Sidhu S, Gomez-Sanchez C, Hellman P, Bjorklund P. Activating mutations in CTNNB1 in aldosterone producing adenomas. Sci Rep. 2016 Jan 27;6:19546. doi: 10.1038/srep19546. Citation on PubMed or Free article on PubMed Central
- Azizan EA, Poulsen H, Tuluc P, Zhou J, Clausen MV, Lieb A, Maniero C, Garg S, Bochukova EG, Zhao W, Shaikh LH, Brighton CA, Teo AE, Davenport AP, Dekkers T, Tops B, Kusters B, Ceral J, Yeo GS, Neogi SG, McFarlane I, Rosenfeld N, Marass F, Hadfield J, Margas W, Chaggar K, Solar M, Deinum J, Dolphin AC, Farooqi IS, Striessnig J, Nissen P, Brown MJ. Somatic mutations in ATP1A1 and CACNA1D underlie a common subtype of adrenal hypertension. Nat Genet. 2013 Sep;45(9):1055-60. doi: 10.1038/ng.2716. Epub 2013 Aug 4. Citation on PubMed
- Beuschlein F, Boulkroun S, Osswald A, Wieland T, Nielsen HN, Lichtenauer UD, Penton D, Schack VR, Amar L, Fischer E, Walther A, Tauber P, Schwarzmayr T, Diener S, Graf E, Allolio B, Samson-Couterie B, Benecke A, Quinkler M, Fallo F, Plouin PF, Mantero F, Meitinger T, Mulatero P, Jeunemaitre X, Warth R, Vilsen B, Zennaro MC, Strom TM, Reincke M. Somatic mutations in ATP1A1 and ATP2B3 lead to aldosterone-producing adenomas and secondary hypertension. Nat Genet. 2013 Apr;45(4):440-4, 444e1-2. doi: 10.1038/ng.2550. Epub 2013 Feb 17. Citation on PubMed
- Choi M, Scholl UI, Yue P, Bjorklund P, Zhao B, Nelson-Williams C, Ji W, Cho Y, Patel A, Men CJ, Lolis E, Wisgerhof MV, Geller DS, Mane S, Hellman P, Westin G, Akerstrom G, Wang W, Carling T, Lifton RP. K+ channel mutations in adrenal aldosterone-producing adenomas and hereditary hypertension. Science. 2011 Feb 11;331(6018):768-72. doi: 10.1126/science.1198785. Citation on PubMed or Free article on PubMed Central
- Fernandes-Rosa FL, Williams TA, Riester A, Steichen O, Beuschlein F, Boulkroun S, Strom TM, Monticone S, Amar L, Meatchi T, Mantero F, Cicala MV, Quinkler M, Fallo F, Allolio B, Bernini G, Maccario M, Giacchetti G, Jeunemaitre X, Mulatero P, Reincke M, Zennaro MC. Genetic spectrum and clinical correlates of somatic mutations in aldosterone-producing adenoma. Hypertension. 2014 Aug;64(2):354-61. doi: 10.1161/HYPERTENSIONAHA.114.03419. Epub 2014 May 27. Citation on PubMed
- Lenzini L, Rossitto G, Maiolino G, Letizia C, Funder JW, Rossi GP. A Meta-Analysis of Somatic KCNJ5 K(+) Channel Mutations In 1636 Patients With an Aldosterone-Producing Adenoma. J Clin Endocrinol Metab. 2015 Aug;100(8):E1089-95. doi: 10.1210/jc.2015-2149. Epub 2015 Jun 11. Citation on PubMed
- Savard S, Amar L, Plouin PF, Steichen O. Cardiovascular complications associated with primary aldosteronism: a controlled cross-sectional study. Hypertension. 2013 Aug;62(2):331-6. doi: 10.1161/HYPERTENSIONAHA.113.01060. Epub 2013 Jun 10. Citation on PubMed
- Scholl UI, Goh G, Stolting G, de Oliveira RC, Choi M, Overton JD, Fonseca AL, Korah R, Starker LF, Kunstman JW, Prasad ML, Hartung EA, Mauras N, Benson MR, Brady T, Shapiro JR, Loring E, Nelson-Williams C, Libutti SK, Mane S, Hellman P, Westin G, Akerstrom G, Bjorklund P, Carling T, Fahlke C, Hidalgo P, Lifton RP. Somatic and germline CACNA1D calcium channel mutations in aldosterone-producing adenomas and primary aldosteronism. Nat Genet. 2013 Sep;45(9):1050-4. doi: 10.1038/ng.2695. Epub 2013 Aug 4. Citation on PubMed or Free article on PubMed Central
- Scholl UI, Lifton RP. New insights into aldosterone-producing adenomas and hereditary aldosteronism: mutations in the K+ channel KCNJ5. Curr Opin Nephrol Hypertens. 2013 Mar;22(2):141-7. doi: 10.1097/MNH.0b013e32835cecf8. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.