

Description
Hirschsprung disease is an intestinal disorder characterized by the absence of nerves in parts of the intestine. This condition occurs when the nerves in the intestine (enteric nerves) do not form properly during development before birth (embryonic development). This condition is usually identified in the first two months of life, although less severe cases may be diagnosed later in childhood.
Enteric nerves trigger the muscle contractions that move stool through the intestine. Without these nerves in parts of the intestine, the material cannot be pushed through, causing severe constipation or complete blockage of the intestine in people with Hirschsprung disease. Other signs and symptoms of this condition include vomiting, abdominal pain or swelling, diarrhea, poor feeding, malnutrition, and slow growth. People with this disorder are at risk of developing more serious conditions such as inflammation of the intestine (enterocolitis) or a hole in the wall of the intestine (intestinal perforation), which can cause serious infection and may be fatal.
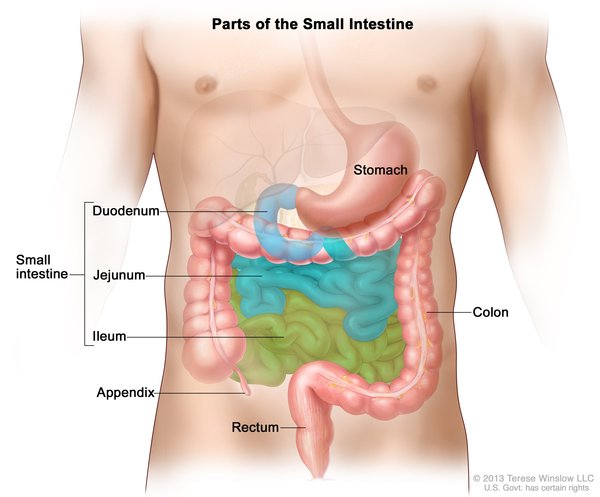
There are two main types of Hirschsprung disease, known as short-segment disease and long-segment disease, which are defined by the region of the intestine lacking nerve cells. In short-segment disease, nerve cells are missing from only the last segment of the large intestine (colon). This type is most common, occurring in approximately 80 percent of people with Hirschsprung disease. For unknown reasons, short-segment disease is four times more common in men than in women. Long-segment disease occurs when nerve cells are missing from most of the large intestine and is the more severe type. Long-segment disease is found in approximately 20 percent of people with Hirschsprung disease and affects men and women equally. Very rarely, nerve cells are missing from the entire large intestine and sometimes part of the small intestine (total colonic aganglionosis) or from all of the large and small intestine (total intestinal aganglionosis).
Hirschsprung disease can occur in combination with other conditions, such as Waardenburg syndrome, type IV; Mowat-Wilson syndrome; or congenital central hypoventilation syndrome. These cases are described as syndromic. Hirschsprung disease can also occur without other conditions, and these cases are referred to as isolated or nonsyndromic.
Frequency
Hirschsprung disease occurs in approximately 1 in 5,000 newborns.
Causes
Isolated Hirschsprung disease can result from mutations in one of several genes, including the RET, EDNRB, and EDN3 genes. However, the genetics of this condition appear complex and are not completely understood. While a mutation in a single gene sometimes causes the condition, mutations in multiple genes may be required in some cases. The genetic cause of the condition is unknown in approximately half of affected individuals.
Mutations in the RET gene are the most common known genetic cause of Hirschsprung disease. The RET gene provides instructions for producing a protein that is involved in signaling within cells. This protein appears to be essential for the normal development of several kinds of nerve cells, including nerves in the intestine. Mutations in the RET gene that cause Hirschsprung disease result in a nonfunctional version of the RET protein that cannot transmit signals within cells. Without RET protein signaling, enteric nerves do not develop properly. Absence of these nerves leads to the intestinal problems characteristic of Hirschsprung disease.
The EDNRB gene provides instructions for making a protein called endothelin receptor type B. When this protein interacts with other proteins called endothelins, it transmits information from outside the cell to inside the cell, signaling for many important cellular processes. The EDN3 gene provides instructions for a protein called endothelin 3, one of the endothelins that interacts with endothelin receptor type B. Together, endothelin 3 and endothelin receptor type B play an important role in the normal formation of enteric nerves. Changes in either the EDNRB gene or the EDN3 gene disrupt the normal functioning of the endothelin receptor type B or the endothelin 3 protein, preventing them from transmitting signals important for the development of enteric nerves. As a result, these nerves do not form normally during embryonic development. A lack of enteric nerves prevents stool from being moved through the intestine, leading to severe constipation and intestinal blockage.
Inheritance
Approximately 20 percent of cases of Hirschsprung disease occur in multiple members of the same family. The remainder of cases occur in people with no history of the disorder in their families.
Hirschsprung disease appears to have a dominant pattern of inheritance, which means one copy of the altered gene in each cell may be sufficient to cause the disorder. The inheritance is considered to have incomplete penetrance because not everyone who inherits the altered gene from a parent develops Hirschsprung disease.

Other Names for This Condition
- Aganglionic megacolon
- Congenital intestinal aganglionosis
- Congenital megacolon
- Hirschsprung's disease
- HSCR
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Scientific Articles on PubMed
References
- Alves MM, Sribudiani Y, Brouwer RW, Amiel J, Antinolo G, Borrego S, Ceccherini I, Chakravarti A, Fernandez RM, Garcia-Barcelo MM, Griseri P, Lyonnet S, Tam PK, van Ijcken WF, Eggen BJ, te Meerman GJ, Hofstra RM. Contribution of rare and common variants determine complex diseases-Hirschsprung disease as a model. Dev Biol. 2013 Oct 1;382(1):320-9. doi: 10.1016/j.ydbio.2013.05.019. Epub 2013 May 23. Citation on PubMed
- Amiel J, Attie T, Jan D, Pelet A, Edery P, Bidaud C, Lacombe D, Tam P, Simeoni J, Flori E, Nihoul-Fekete C, Munnich A, Lyonnet S. Heterozygous endothelin receptor B (EDNRB) mutations in isolated Hirschsprung disease. Hum Mol Genet. 1996 Mar;5(3):355-7. doi: 10.1093/hmg/5.3.355. Citation on PubMed
- Edery P, Lyonnet S, Mulligan LM, Pelet A, Dow E, Abel L, Holder S, Nihoul-Fekete C, Ponder BA, Munnich A. Mutations of the RET proto-oncogene in Hirschsprung's disease. Nature. 1994 Jan 27;367(6461):378-80. doi: 10.1038/367378a0. Citation on PubMed
- Jiang Q, Arnold S, Heanue T, Kilambi KP, Doan B, Kapoor A, Ling AY, Sosa MX, Guy M, Jiang Q, Burzynski G, West K, Bessling S, Griseri P, Amiel J, Fernandez RM, Verheij JB, Hofstra RM, Borrego S, Lyonnet S, Ceccherini I, Gray JJ, Pachnis V, McCallion AS, Chakravarti A. Functional loss of semaphorin 3C and/or semaphorin 3D and their epistatic interaction with ret are critical to Hirschsprung disease liability. Am J Hum Genet. 2015 Apr 2;96(4):581-96. doi: 10.1016/j.ajhg.2015.02.014. Citation on PubMed or Free article on PubMed Central
- Lecerf L, Kavo A, Ruiz-Ferrer M, Baral V, Watanabe Y, Chaoui A, Pingault V, Borrego S, Bondurand N. An impairment of long distance SOX10 regulatory elements underlies isolated Hirschsprung disease. Hum Mutat. 2014 Mar;35(3):303-7. doi: 10.1002/humu.22499. Epub 2014 Jan 8. Citation on PubMed
- Natarajan D, Marcos-Gutierrez C, Pachnis V, de Graaff E. Requirement of signalling by receptor tyrosine kinase RET for the directed migration of enteric nervous system progenitor cells during mammalian embryogenesis. Development. 2002 Nov;129(22):5151-60. doi: 10.1242/dev.129.22.5151. Citation on PubMed
- Pasini B, Borrello MG, Greco A, Bongarzone I, Luo Y, Mondellini P, Alberti L, Miranda C, Arighi E, Bocciardi R, et al. Loss of function effect of RET mutations causing Hirschsprung disease. Nat Genet. 1995 May;10(1):35-40. doi: 10.1038/ng0595-35. Citation on PubMed
- Svensson PJ, Von Tell D, Molander ML, Anvret M, Nordenskjold A. A heterozygous frameshift mutation in the endothelin-3 (EDN-3) gene in isolated Hirschsprung's disease. Pediatr Res. 1999 May;45(5 Pt 1):714-7. doi: 10.1203/00006450-199905010-00018. Citation on PubMed
- Tam PK, Garcia-Barcelo M. Genetic basis of Hirschsprung's disease. Pediatr Surg Int. 2009 Jul;25(7):543-58. doi: 10.1007/s00383-009-2402-2. Epub 2009 Jun 12. Citation on PubMed
- Wallace AS, Anderson RB. Genetic interactions and modifier genes in Hirschsprung's disease. World J Gastroenterol. 2011 Dec 7;17(45):4937-44. doi: 10.3748/wjg.v17.i45.4937. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.