

Description
Primary macronodular adrenal hyperplasia (PMAH) is a disorder characterized by multiple lumps (nodules) in the adrenal glands, which are small hormone-producing glands located on top of each kidney. These nodules, which usually are found in both adrenal glands (bilateral) and vary in size, cause adrenal gland enlargement (hyperplasia) and result in the production of higher-than-normal levels of the hormone cortisol. Cortisol is an important hormone that suppresses inflammation and protects the body from physical stress such as infection or trauma through several mechanisms including raising levels of blood glucose, also called blood sugar.
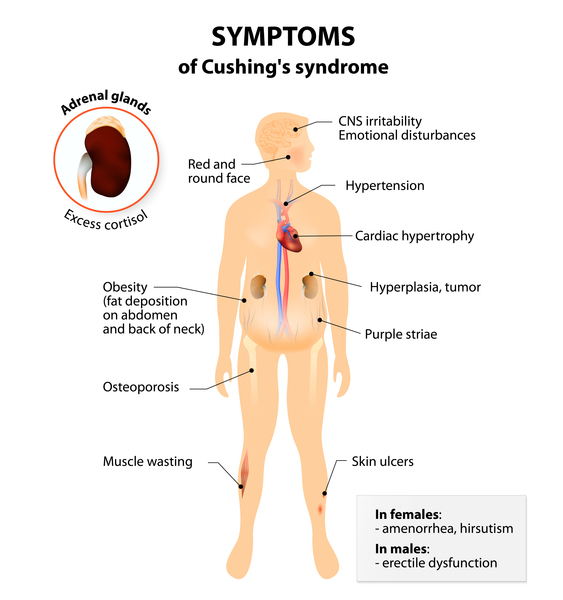
PMAH typically becomes evident in a person's forties or fifties. It is considered a form of Cushing syndrome, which is characterized by increased levels of cortisol resulting from one of many possible causes. These increased cortisol levels lead to weight gain in the face and upper body, fragile skin, bone loss, fatigue, and other health problems. However, some people with PMAH do not experience these signs and symptoms and are said to have subclinical Cushing syndrome.
Frequency
PMAH is a rare disorder. It is present in less than 1 percent of cases of endogenous Cushing syndrome, which describes forms of Cushing syndrome caused by factors internal to the body rather than by external factors such as long-term use of certain medicines called corticosteroids. The prevalence of endogenous Cushing syndrome is about 1 in 26,000 people.
Causes
In about half of individuals with PMAH, the condition is caused by mutations in the ARMC5 gene. This gene provides instructions for making a protein that is thought to act as a tumor suppressor, which means that it helps to prevent cells from growing and dividing too rapidly or in an uncontrolled way. ARMC5 gene mutations are believed to impair the protein's tumor-suppressor function, which allows the overgrowth of certain cells. It is unclear why this overgrowth is limited to the formation of adrenal gland nodules in people with PMAH.
PMAH can also be caused by mutations in the GNAS gene. This gene provides instructions for making one component, the stimulatory alpha subunit, of a protein complex called a guanine nucleotide-binding protein (G protein). The G protein produced from the GNAS gene helps stimulate the activity of an enzyme called adenylate cyclase. This enzyme is involved in controlling the production of several hormones that help regulate the activity of certain endocrine glands, including the adrenal glands. The GNAS gene mutations that cause PMAH are believed to result in an overactive G protein. Research suggests that the overactive G protein may increase levels of adenylate cyclase and result in the overproduction of another compound called cyclic AMP (cAMP). An excess of cAMP may trigger abnormal cell growth and lead to the adrenal nodules characteristic of PMAH.
Mutations in other genes, some of which are unknown, can also cause PMAH.
Inheritance
People with PMAH caused by ARMC5 gene mutations inherit one copy of the mutated gene in each cell. The inheritance is considered autosomal dominant because one copy of the mutated gene is sufficient to make an individual susceptible to PMAH. However, the condition develops only when affected individuals acquire another mutation in the other copy of the ARMC5 gene in certain cells of the adrenal glands. This second mutation is described as somatic. Instead of being passed from parent to child, somatic mutations are acquired during a person's lifetime and are present only in certain cells. Because somatic mutations are also required for PMAH to occur, some people who have inherited the altered ARMC5 gene never develop the condition, a situation known as reduced penetrance.

When PMAH is caused by GNAS gene mutations, the condition is not inherited. The GNAS gene mutations that cause PMAH are somatic mutations. In PMAH, the gene mutation is believed to occur early in embryonic development. Cells with the mutated GNAS gene can be found in both adrenal glands.
Other Names for This Condition
- ACTH-independent macronodular adrenal hyperplasia
- ACTH-independent macronodular adrenocortical hyperplasia
- Adrenal Cushing syndrome due to AIMAH
- Adrenocorticotropic hormone-independent macronodular adrenal hyperplasia
- AIMAH
- Corticotropin-independent macronodular adrenal hyperplasia
- PMAH
- Primary bilateral macronodular adrenal hyperplasia
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Alencar GA, Lerario AM, Nishi MY, Mariani BM, Almeida MQ, Tremblay J, Hamet P, Bourdeau I, Zerbini MC, Pereira MA, Gomes GC, Rocha Mde S, Chambo JL, Lacroix A, Mendonca BB, Fragoso MC. ARMC5 mutations are a frequent cause of primary macronodular adrenal Hyperplasia. J Clin Endocrinol Metab. 2014 Aug;99(8):E1501-9. doi: 10.1210/jc.2013-4237. Epub 2014 Apr 7. Citation on PubMed
- Assie G, Libe R, Espiard S, Rizk-Rabin M, Guimier A, Luscap W, Barreau O, Lefevre L, Sibony M, Guignat L, Rodriguez S, Perlemoine K, Rene-Corail F, Letourneur F, Trabulsi B, Poussier A, Chabbert-Buffet N, Borson-Chazot F, Groussin L, Bertagna X, Stratakis CA, Ragazzon B, Bertherat J. ARMC5 mutations in macronodular adrenal hyperplasia with Cushing's syndrome. N Engl J Med. 2013 Nov 28;369(22):2105-14. doi: 10.1056/NEJMoa1304603. Citation on PubMed or Free article on PubMed Central
- De Venanzi A, Alencar GA, Bourdeau I, Fragoso MC, Lacroix A. Primary bilateral macronodular adrenal hyperplasia. Curr Opin Endocrinol Diabetes Obes. 2014 Jun;21(3):177-84. doi: 10.1097/MED.0000000000000061. Citation on PubMed
- Elbelt U, Trovato A, Kloth M, Gentz E, Finke R, Spranger J, Galas D, Weber S, Wolf C, Konig K, Arlt W, Buttner R, May P, Allolio B, Schneider JG. Molecular and clinical evidence for an ARMC5 tumor syndrome: concurrent inactivating germline and somatic mutations are associated with both primary macronodular adrenal hyperplasia and meningioma. J Clin Endocrinol Metab. 2015 Jan;100(1):E119-28. doi: 10.1210/jc.2014-2648. Citation on PubMed or Free article on PubMed Central
- Faucz FR, Zilbermint M, Lodish MB, Szarek E, Trivellin G, Sinaii N, Berthon A, Libe R, Assie G, Espiard S, Drougat L, Ragazzon B, Bertherat J, Stratakis CA. Macronodular adrenal hyperplasia due to mutations in an armadillo repeat containing 5 (ARMC5) gene: a clinical and genetic investigation. J Clin Endocrinol Metab. 2014 Jun;99(6):E1113-9. doi: 10.1210/jc.2013-4280. Epub 2014 Mar 6. Citation on PubMed or Free article on PubMed Central
- Fragoso MC, Domenice S, Latronico AC, Martin RM, Pereira MA, Zerbini MC, Lucon AM, Mendonca BB. Cushing's syndrome secondary to adrenocorticotropin-independent macronodular adrenocortical hyperplasia due to activating mutations of GNAS1 gene. J Clin Endocrinol Metab. 2003 May;88(5):2147-51. doi: 10.1210/jc.2002-021362. Citation on PubMed
- Gagliardi L, Schreiber AW, Hahn CN, Feng J, Cranston T, Boon H, Hotu C, Oftedal BE, Cutfield R, Adelson DL, Braund WJ, Gordon RD, Rees DA, Grossman AB, Torpy DJ, Scott HS. ARMC5 mutations are common in familial bilateral macronodular adrenal hyperplasia. J Clin Endocrinol Metab. 2014 Sep;99(9):E1784-92. doi: 10.1210/jc.2014-1265. Epub 2014 Jun 6. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.