

Description
Systemic mastocytosis is a blood disorder that can affect many different body systems. Individuals with the condition can develop signs and symptoms at any age, but it usually appears after adolescence.
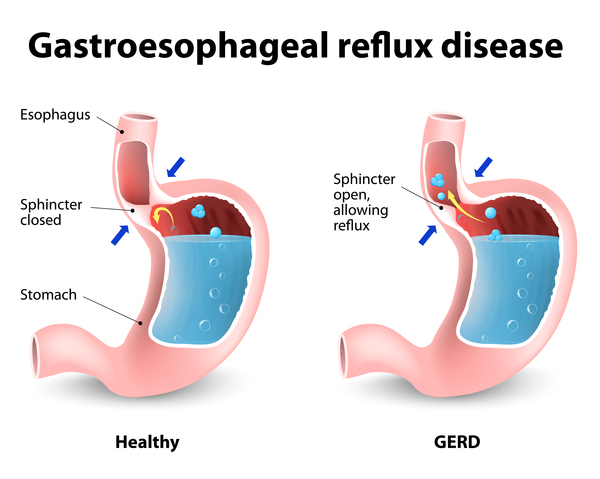
Signs and symptoms of systemic mastocytosis often include extreme tiredness (fatigue), skin redness and warmth (flushing), nausea, abdominal pain, bloating, diarrhea, the backflow of stomach acids into the esophagus (gastroesophageal reflux), nasal congestion, shortness of breath, low blood pressure (hypotension), lightheadedness, and headache. Some affected individuals have attention or memory problems, anxiety, or depression. Many individuals with systemic mastocytosis develop a skin condition called urticaria pigmentosa, which is characterized by raised patches of brownish skin that sting or itch with contact or changes in temperature. Nearly half of individuals with systemic mastocytosis will experience severe allergic reactions (anaphylaxis).
There are five subtypes of systemic mastocytosis, which are differentiated by their severity and the signs and symptoms. The mildest forms of systemic mastocytosis are the indolent and smoldering types. Individuals with these types tend to have only the general signs and symptoms of systemic mastocytosis described above. Individuals with smoldering mastocytosis may have more organs affected and more severe features than those with indolent mastocytosis. The indolent type is the most common type of systemic mastocytosis.
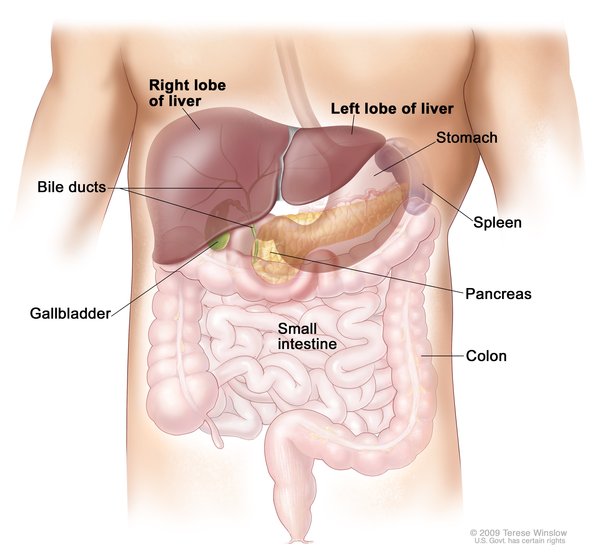
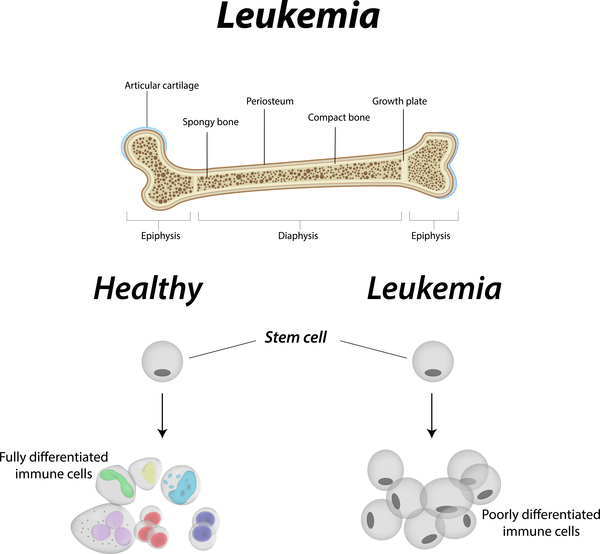
The severe types include aggressive systemic mastocytosis, systemic mastocytosis with an associated hematologic neoplasm, and mast cell leukemia. These types are associated with a reduced life span, which varies among the types and affected individuals. In addition to the general signs and symptoms of systemic mastocytosis, these types typically involve impaired function of an organ, such as the liver, spleen, or lymph nodes. The organ dysfunction can result in an abnormal buildup of fluid in the abdominal cavity (ascites). Aggressive systemic mastocytosis is associated with a loss of bone tissue (osteoporosis and osteopenia) and multiple bone fractures. Systemic mastocytosis with an associated hematologic neoplasm and mast cell leukemia both involve blood cell disorders or blood cell cancer (leukemia). Mast cell leukemia is the rarest and most severe type of systemic mastocytosis.
Individuals with the milder forms of the condition generally have a normal or near normal life expectancy, while those with the more severe forms typically survive months or a few years after diagnosis.
Frequency
Systemic mastocytosis is estimated to occur in 1 per 10,000 to 20,000 individuals worldwide.
Causes
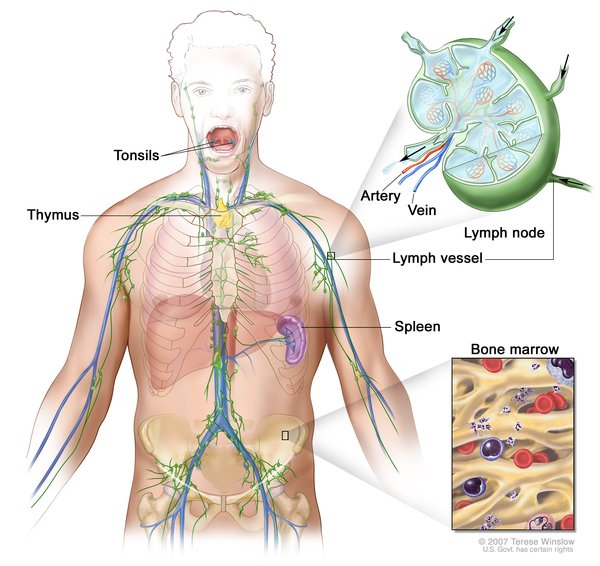
Systemic mastocytosis occurs when white blood cells called mast cells, which are produced in bone marrow, abnormally accumulate in one or more tissues. In most cases of systemic mastocytosis, the accumulated mast cells have a mutation in a gene called KIT. The KIT gene provides instructions for making a protein that plays an important role in development and activity of mast cells. The KIT protein stimulates chemical signaling pathways that are involved in the growth and division (proliferation) of many types of cells, including mast cells. In systemic mastocytosis, KIT gene mutations are somatic, which means they are acquired during a person's lifetime. These mutations result in a KIT protein that is always turned on (activated). As a result, signaling pathways are overactive, leading to increased production and accumulation of mast cells.
In systemic mastocytosis, mast cells most often accumulate in the bone marrow, which is where new blood cells are made. Mast cells can also gather in other tissues such as the gastrointestinal tract, lymph nodes, spleen, or liver. In severe cases, excessive accumulation of mast cells can interfere with normal organ functioning. Mast cells normally trigger inflammation during an allergic reaction. When mast cells are activated by an environmental trigger, they release proteins (called mediators) that signal an immune response. In systemic mastocytosis, excess mast cells mean more mediator proteins are being released in the tissues where the cells accumulate, leading to an increased immune response. In affected individuals, triggers that can activate mast cells include changes in temperature, friction and minor trauma, surgery, insect stings, vaccines, anxiety, and stress. Certain medications can also be triggers, including aspirin, opioids, or non-steroidal anti-inflammatory drugs (NSAIDs).
Mutations in additional genes seem to modify the severity of systemic mastocytosis, often resulting in a more aggressive disease and shorter survival. These genes primarily play roles in controlling the proliferation of cells or regulating the activity of other genes that are important in development.
Inheritance
This condition is generally not inherited but arises from a somatic mutation in the body's cells that occurs after conception.
Other Names for This Condition
- Mast cell disease, systemic
- Mastocytosis, systemic
- Systemic mast cell disease
- Systemic mast-cell disease
- Systemic mastocytoses
- Systemic tissue mast cell disease
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Akin C, Valent P. Diagnostic criteria and classification of mastocytosis in 2014. Immunol Allergy Clin North Am. 2014 May;34(2):207-18. doi: 10.1016/j.iac.2014.02.003. Citation on PubMed
- Bonadonna P, Pagani M, Aberer W, Bilo MB, Brockow K, Oude Elberink H, Garvey L, Mosbech H, Romano A, Zanotti R, Torres MJ. Drug hypersensitivity in clonal mast cell disorders: ENDA/EAACI position paper. Allergy. 2015 Jul;70(7):755-63. doi: 10.1111/all.12617. Epub 2015 Apr 24. Citation on PubMed
- Castells MC. Mastocytosis: Moving the Field to Precision and Personalized Medicine. Immunol Allergy Clin North Am. 2018 Aug;38(3):xv-xvii. doi: 10.1016/j.iac.2018.05.001. Epub 2018 Jun 9. No abstract available. Citation on PubMed
- Scherber RM, Borate U. How we diagnose and treat systemic mastocytosis in adults. Br J Haematol. 2018 Jan;180(1):11-23. doi: 10.1111/bjh.14967. Epub 2017 Oct 19. Citation on PubMed
- Tremblay D, Carreau N, Kremyanskaya M, Mascarenhas J. Systemic Mastocytosis: Clinical Update and Future Directions. Clin Lymphoma Myeloma Leuk. 2015 Dec;15(12):728-38. doi: 10.1016/j.clml.2015.07.644. Epub 2015 Aug 5. Citation on PubMed
- Valent P, Aberer E, Beham-Schmid C, Fellinger C, Fuchs W, Gleixner KV, Greul R, Hadzijusufovic E, Hoermann G, Sperr WR, Wimazal F, Wohrl S, Zahel B, Pehamberger H. Guidelines and diagnostic algorithm for patients with suspected systemic mastocytosis: a proposal of the Austrian competence network (AUCNM). Am J Blood Res. 2013 May 5;3(2):174-80. Print 2013. Citation on PubMed or Free article on PubMed Central
- Valent P, Akin C, Metcalfe DD. Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts. Blood. 2017 Mar 16;129(11):1420-1427. doi: 10.1182/blood-2016-09-731893. Epub 2016 Dec 28. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.